In our commercial sector, customers are placing increased demands on companies for high quality, reliable products. The increasing capabilities and functionality of many products are making it more difficult for manufacturers to maintain the quality and reliability. Traditionally, reliability has been achieved through extensive testing and use of techniques such as probabilistic reliability modeling. These are techniques done in the late stages of development. The challenge is to design in quality and reliability early in the development cycle.
Failure Modes and Effects Analysis (FMEA) is a methodology for analyzing potential reliability problems early in the development cycle where it is easier to take actions to overcome these issues, thereby enhancing reliability through design. FMEA is used to identify potential failure modes, determine their effect on the operation of the product, and identify actions to mitigate the failures. A crucial step is anticipating what might go wrong with a product. While anticipating every failure mode is not possible, the development team should formulate as extensive a list of potential failure modes as possible.
The early and consistent use of FMEAs in the design process allows the engineer to design out failures and produce reliable, safe, and customer pleasing products and services. FMEAs also capture historical information for use in future product improvement. FMEA has become a standard tool for both engineering design and process analysis. It has proven to be of great value in the early identification of potential reliability and safety issues. It is beginning to be used in the healthcare industry to improve services and products.
There are several types of FMEAs, some are used much more often than others. FMEAs should always be performed for engineered systems whenever failures would mean potential harm or injury to the user of the end item being designed. The types of FMEA are:
Historically, engineers and healthcare providers have done a good job of evaluating the functions and the form of products and processes in the design phase. They have not always done so well at designing in reliability and quality. Often the engineer (and now the healthcare provider) uses safety factors as a way of making sure that the design or treatment will work and protect the user against product or process failure. As described in a recent article:
"A large safety factor does not necessarily translate into a reliable product. Instead, it often leads to an over-designed product with reliability problems."
Failure Analysis Beats Murphy's Law
Mechanical Engineering , September 1993
FMEA's provide us with a tool that can assist in providing reliable, safe, and customer pleasing products and processes. Since FMEA help us to identify potential product or process failures, they can use it to:
FMEA is designed to assist the engineer improve the quality and reliability of design. Properly used the FMEA provides the engineer several benefits. Among others, these benefits include:
The FMEA is a living document. Throughout the product development cycle change and updates are made to the product and process. These changes can and often do introduce new failure modes. It is therefore important to review and/or update the FMEA when:
The process for conducting an FMEA is straightforward. The basic steps are outlined below.
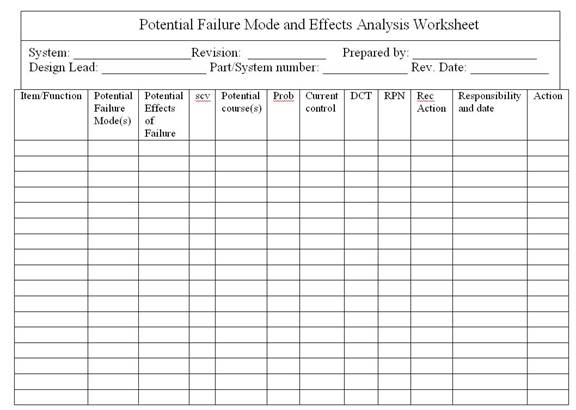
Establish a numerical ranking for the severity of the effect. A common industry standard scale uses 1 to represent no effect and 10 to indicate very severe with failure affecting system operation and safety without warning. The intent of the ranking is to help the analyst determine whether a failure would be a minor nuisance or a catastrophic occurrence to the customer. This enables the engineer to prioritize the failures and address the real big issues first.
For the Calgary Health Region (CHR), patient safety was brought to the forefront in the spring of 2004, when there were two critical incidents that resulted in the death of two patients receiving CRRT in two different ICUs of the CHR (ISMP alert March 25, 2004). Here is a brief description of the incidents from the External Patient Safety Review (June 2004):
" An 83-year-old woman who was a patient in the cardio-vascular care unit at the Foothills Medical Center (FMC) site of the CHR died suddenly in the presence of her physician and members of her family. She was alert and oriented at the time and her condition, while very serious, did not seem to indicate reasons for immediate concern. Her unexpected death was devastating for her family and extremely distressing for all those involved in her care. An ICU physician suspected the cause - the composition of dialysate solution being used to treat her kidney failure. This was quickly confirmed and 30 bags of the solution made in the same batch were removed from patient care areas, undoubtedly preventing the deaths of other patients. An analysis of the other bags from that batch as well as a systematic review of patient records identified a second patient whose death, one week earlier, was likely caused by the same set of circumstances. This was not suspected at the time of death due to the patient's serious condition."
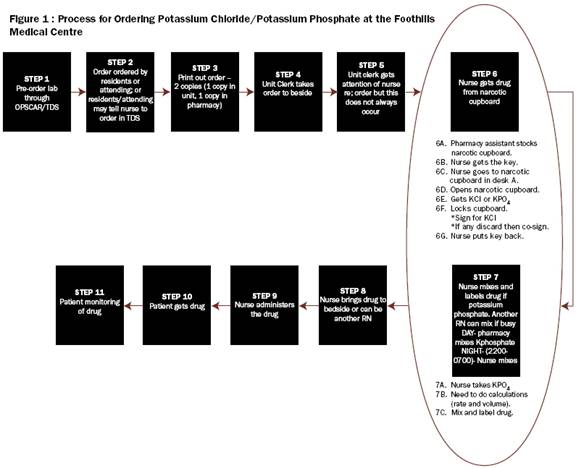
Upon further investigation, it was determined that in February 2004, pharmacy technicians in the central production facility of the CHR pharmacy department prepared a dialysate solution for patients receiving CRRT. During the process, KCL was inadvertently added to the dialysate bags instead of sodium chloride (NaCl) solution. It is believed that these incorrectly prepared solutions were used in the dialysis of the two patients who died (External Patient Safety Review, CHR June 2004).
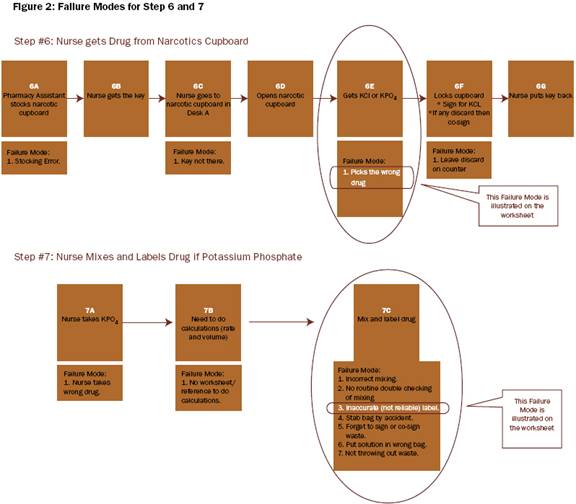
The CHR publicly disclosed the facts and initiated an external patient safety review. The Department of Critical Care Medicine (DCCM) also undertook a review of the process for ordering and administering intravenous, high-concentration KCl and KPO4, using the HFMEA tool developed by DeRosier, Joseph et al. (2002). The focus of this article is to describe the application of the tool with respect to reviewing the processes involved in ordering and administering intravenous, high-concentration KCl and KPO4, thereby allowing the DCCM to proactively identify hazards that may exist and establish a safer process.
The DCCM has been engaged in ongoing quality improvement and patient safety initiatives both formally and informally for over 10 years (Esmail et al. 2005). At present, the region includes three adult acute care teaching hospitals and one pediatric hospital: Foothills Medical Centre (FMC), Peter Lougheed Center (PLC), Rockyview General Hospital (RGH) and the Alberta Children's Hospital. The Department of Critical Care Medicine oversees four adult intensive care units:
In the past, medicine used a human error approach which identified the individual as the cause of the adverse event. We now recognize that errors are caused by system or process failures (McNally et al. 1997). FMEA was developed for use by the United States military and is utilized by the National Aeronautics and Space Administration (NASA), to predict and evaluate potential failures and unrecognized hazards and to proactively identify steps in a process that could help reduce or eliminate a failure from occurring (Reiling et al. 2003). FMEA focuses on the system within an environment and uses a multidisciplinary team to evaluate a process from a quality improvement perspective. The Joint Commission for Accreditation of Healthcare Organizations (JCAHO) in the US has recommended that healthcare institutions conduct proactive risk management activities that identify and predict system weaknesses and adopt changes to minimize patient harm (Adachi et al. 2001).
In 2001 the Veteran's Administration (VA) National Centre for Patient Safety (NCPS) specifically designed the HFMEA tool for risk assessment in the healthcare field.
The HFMEA tool was formed by combining industry's FMEA model with the U.S. Food and Drug Administration's Hazard Analysis and Critical Control Point (HACCP) tool together with components from the VA's root cause analysis (RCA) process. HACCP was developed to protect food from chemical and biological contamination and physical hazards. The HACCP system uses seven steps: (1) conduct a hazard analysis, (2) identify critical control points, (3) establish critical limits, (4) establish monitoring procedures, (5) establish corrective actions, (6) establish verification procedures, and (7) establish record-keeping and documentation procedures (Center for Food Safety and Applied Nutrition, 1997). It uses questions to probe for food system vulnerabilities as well as a decision tree to identify critical control points. The decision tree concept was adapted by the VA for the HFMEA tool. The HFMEA tool has been subsequently recognized in the White Paper prepared by the American Society for Healthcare Risk Management (ASHRM). In an effort to globally share the merits of this process, a video, instructional CD and worksheets on the use and application of HFMEA has been sent to every hospital CEO in the US to be shared with individuals and risk managers responsible for patient safety (American Society for Health Risk Management 2002).
Step one is to define the HFMEA topic. The topic is usually a process that has high vulnerabilities and potential for impacting patient safety. It is important in a HFMEA analysis to define boundaries and limit the scope of the topic being reviewed.
Following the two previously mentioned critical incidents, two reviews were conducted in the CHR. The first was an internal review and was conducted by the Patient Safety Task Force, and the second was considered external and performed by the External Patient Safety Review Committee (June 2004). During the same time, in response to the tragic events from March 2004, disparate and poorly coordinated changes in policy regarding the storage and use of highly concentrated potassium were initiated within the regional ICUs. The department's ICU executive council determined the need to undertake a review of the process for the general handling of intravenous, high-concentration KCl and KPO4 prior to reviewing the process of preparing CRRT bags for dialysis. It was understood that some of the steps in this process would overlap with the CRRT process.
Step two in the HFMEA tool is to assemble a team. The team should include six to eight multidisciplinary members who are involved in the process being analyzed and are to some degree considered "subject matter" experts.
The department's PSAT was assigned this task. The team was co-led by an intensivist and the department's quality improvement and patient safety consultant. The team was multidisciplinary, with two intensivists, three respiratory therapists, two nursing educators, two frontline nursing staff from each hospital site and two pharmacists. The team had been previously working on chart reviews of adverse events using the IHI trigger tool methodology (Rozich et al. 2003) and staff education with respect to incidents and incident reporting. The team met every other week over a two-month period (April and May 2004).
In step five of the HFMEA tool, actions are developed. Actions to address the identified hazards need to focus on root causes or contributing factors and need to be specific and concrete. Frontline staff involved directly in the process need to review them. Actions can then be tested prior to implementation using the Improvement Model methodology that includes testing changes using the Plan-Do-Study-Act (PDSA) cycle (Langley et al. 1996). Outcomes must be measurable, with a defined sampling strategy, set timeframe for measurement and with a realistic well-articulated goal.
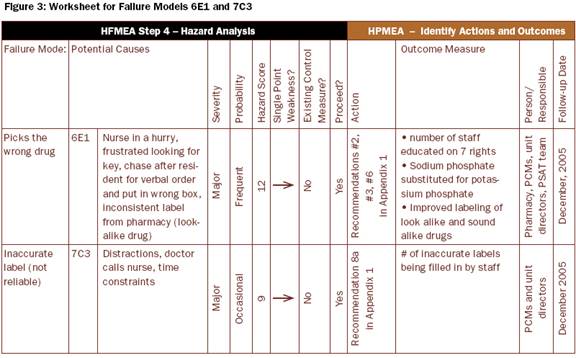
Eleven recommendations were developed based on this analysis (Appendix I). These recommendations were placed into two categories, general and ICU-specific, and subsequently presented to the ICU executive council in July 2004. These recommendations addressed how KCl and KPO4 are to be stored and who, where, and how the drugs are to be mixed. These recommendations also focused on the identification of look-alike and sound-alike products based on human factor principles (Gosbee et al. 2002 and Wickens et al. 2004). Key recommendations were summarized into an action plan with delegated responsibility and timelines for implementation (Figure 3).
HFMEA was well recognized by the PSAT and it provided a solid framework for the step-by-step analysis of potassium ordering and administration. The team members were unaware of the numerous steps involved in administrating this medication and it became obvious that there were many opportunities for errors to occur. HFMEA enabled the team to prioritize the critical items of a complex process and took the subjectivity out of the analysis.
The multidisciplinary structure of PSAT allowed members to identify each step from their own professional practice perspective. The PSAT composition also generated diverse ideas when brainstorming actions and allowed for good discussion and deliberation, which ultimately promoted team building.
HFMEA was an easy tool to use by all members of the team. It made the approach to a very complicated process relatively straightforward. Using the HFMEA tool, the two leaders were able to focus the team on the specific components of the tool. The tool enabled the team to develop a structured outline of the goals that needed to be accomplished at each meeting. The team has also used this tool to analyze the hazards of the process for preparing CRRT bags for dialysis patients in the ICU.
Although the work of the PSAT was extremely valuable for the department, it was also time consuming. It would be appropriate to conduct a HFMEA analysis on one or two high-priority topics per year as has been recommended by the Joint Commission on Accreditation of Health Care Organizations in the United States (Adachi et al. 2001).
The dialysate manufacturing error came as a harsh reminder to the CHR's pharmacy department of its need for structured policies and procedures for error avoidance. This error occurred despite existing safety procedures that including four double checks by pharmacists. The risks associated with intravenous potassium came to the forefront of the pharmacy department's focus and there was a heightened awareness of pharmacy's role in patient safety.
Since 2002, intravenous high concentration KCL vials have not been available in most patient care areas in the CHR. Premixed KCL bags are available and any special bags not commercially available are to be mixed in the pharmacy department. These policies are based on the ISMP Canada recommendations (2002) and also reiterated in the PSAT recommendations. Prior to the incidents, intravenous potassium vials were available in the night dispensary for use while the pharmacy was closed; these have now been replaced by premixed bags. The only vials of intravenous potassium available outside the pharmacy department include a small supply of KCl vials kept in narcotic cupboards of critical care and dialysis units. These vials are to be used for special CRRT solutions only.
Before the dialysate manufacturing error occurred, intra-venous potassium vials were stored on the regular drug shelves within the pharmacy department. Since the error, all intra-venous potassium vials are stored in a separate, locked area within the pharmacy. All intravenous potassium vials and minibags are now labelled with a warning sticker to further distinguish them, as per the recommendation from ISMP Canada (ISMP alert 2002).
Additionally, drug identification numbers have been added to the manufacturing worksheets used by pharmacy technicians in the sterile product preparation area. This adds redundancy through checking of the procedure for sterile products, including dialysate. Batches of dialysate are now quarantined until potassium levels in each batch are confirmed to be zero by laboratory testing.
By changing preparation, manufacturing, labeling and storage procedures for intravenous potassium products, the risk of error has been substantially reduced.
This article described the use of the HFMEA tool developed by the VA and its application in the process of ordering and administrating intravenous high-concentration KCL and KPO4. Eleven recommendations resulted from this analysis. The ICU-specific recommendations that did not incur costs were implemented expeditiously. General recommendations, which were not under the purview of the DCCM, were shared with CHR's Regional Patient Safety Committee, which has since developed a regional policy on KCl.
In addition to this work, the knowledge and understanding gained from the application of the HFMEA tool by DCCM's PSAT will be shared with the Regional Patient Safety Transport working group reviewing patient transport between hospitals. This group has been formed based on recommendations from the External Patient Safety Review (June 2004). The Quality, Safety & Health Information Portfolio of the region is also in the process of determining the use or modification of this tool to proactively identify hazards in the system.
More importantly, the two critical incidents served as triggers that brought patient safety to the forefront for the CHR and the DCCM. Numerous changes and initiatives based on the recommendations from the internal and external reviews have been initiated or are underway with an attempt to transform the culture of the organization to one with a much greater awareness of hazard identification, incident and near miss reporting and patient safety.
General/ICU
1. Use premixed solutions for high-risk drugs as much as possible.
General/ICU
2. Education, to re-emphasize the 5 (7) RIGHTS of drug administration: Right patient, right drug, right dose, right route, and right time, and,
Right reason and right documentation.
General
3. Concentrated potassium solutions (high-concentrated vials) are removed from ward stock and the night pharmacy.
ICU
ICU
4a. Better identification and storage of the various minibags, with large colour-coded labels used.
ICU
4b. Reduce the range of premixed potassium solutions available.
General/ICU
4c. If possible, use oral potassium supplements in lieu of intravenous solutions.
ICU
5a. In the FMC site, the "A" medication area is moved away from the unit clerk's desk. At the RGH site, medication area moved or renovated to decrease noise and distractions.
General/ICU
5b. Educate and encourage a do not disturb policy when medications are being mixed.
General/ICU
6. Look-alike and sound-alike drugs are highlighted better.
ICU
7. When boluses of potassium are being given the orders and medication be double-checked and charted in QS. This should include patients receiving boluses of 40 mmols or greater or when the ICU K protocol is used.
General/ICU
8a. When medications are mixed in the ICU or on the ward, proper labelling is to include patient name, drug, concentration, date/time and who mixed the medication.
ICU
8b. A standardized protocol is developed and implemented for the administration and monitoring of potassium replacement in severe life threatening hypokalemia.
General/ICU
9a. Clear and simple instructions for mixing a solution are included in the region's intravenous therapy manual.
General
10. Consider using satellite pharmacies in areas where high-risk drugs are used.
ICU
9b. Use a "keypad box" for the narcotics key at the FMC site. (Currently used at the PLC and RGH.)
General
11. Immediate changes to the TDS order sets are made.
Source: http://www.engr.psu.edu/cim/IE497/HEALTFAILURE%20MODE%20EFFECTS%20ANALYSIS.doc
Web site to visit: http://www.engr.psu.edu
Author of the text: indicated on the source document of the above text
If you are the author of the text above and you not agree to share your knowledge for teaching, research, scholarship (for fair use as indicated in the United States copyrigh low) please send us an e-mail and we will remove your text quickly. Fair use is a limitation and exception to the exclusive right granted by copyright law to the author of a creative work. In United States copyright law, fair use is a doctrine that permits limited use of copyrighted material without acquiring permission from the rights holders. Examples of fair use include commentary, search engines, criticism, news reporting, research, teaching, library archiving and scholarship. It provides for the legal, unlicensed citation or incorporation of copyrighted material in another author's work under a four-factor balancing test. (source: http://en.wikipedia.org/wiki/Fair_use)
The information of medicine and health contained in the site are of a general nature and purpose which is purely informative and for this reason may not replace in any case, the council of a doctor or a qualified entity legally to the profession.
The texts are the property of their respective authors and we thank them for giving us the opportunity to share for free to students, teachers and users of the Web their texts will used only for illustrative educational and scientific purposes only.
All the information in our site are given for nonprofit educational purposes